The goal of this collaboration between mathematicians and a healthcare centre is to reduce the number of patients that are refused by the surgery/anaesthesia team after being referred for ambulatory surgery by the general practitioner. These events lead to a significant delay on the surgery time for each refused patient, as an inpatient care surgery as to be scheduled from a fresh start. This project provided the healthcare centre with a new mathematical tool, which will allow the general practitioner to predict, with strong accuracy, the probability of a given patient to be rejected for an ambulatory surgery.
Challenge overview
CHUPORTO (Centro Hospitalar Universitário do Porto) identified a significant rate of patients who were refused by the surgical team after being signalled for ambulatory surgery by the general practitioner. To overcome this problem, a team of surgeons contacted LEMA (Laboratory for Mathematical Engineering at the School of Engineering of the Polytechnic Institute of Porto) asking if mathematical modelling could help in this particular situation.
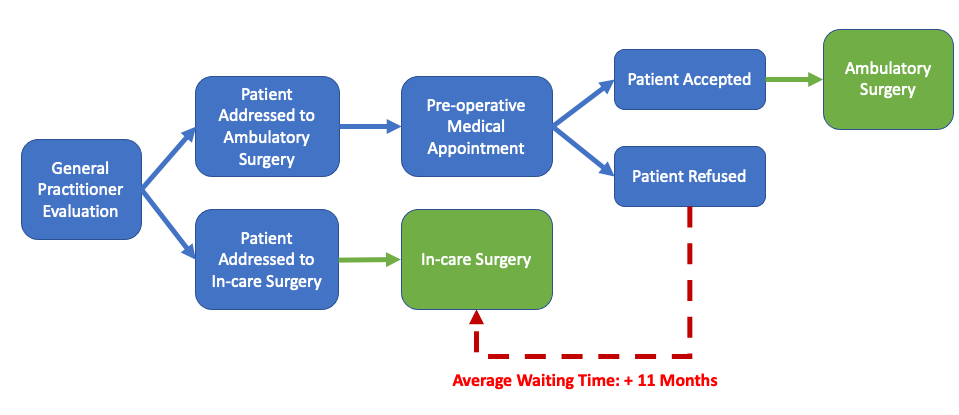
The problem can be briefly described. After the initial referral by the general practitioner, the patient is admitted for a pre-operative medical appointment by the ambulatory surgeon. Based on this initial assessment, the patient is either proposed for evaluation by the anaesthesiologist or refused for ambulatory surgery and referenced for inpatient treatment. When being evaluated by the anaesthesiologist, the patient can also be accepted or refused for ambulatory surgery. There are no established clinical guidelines for refusal. Indeed, these decisions are based on each patient basis.
The ability to define with a certain degree of certainty those patients who are likely to be refused for ambulatory surgery would be valuable as this imposes a delay in the resolution of the patients’ condition with added days of morbidity, increased loss of both working days and healthcare costs. Thus, the team of surgeons from CHUPORTO and mathematicians from LEMA agreed to develop a tailor-made mathematical model, which allows the general practitioner to parameterize the amount of risk they wish to assume in terms of the probability of refusal for a given patient. This model returns, based on previous patient records, the expected probability of refusal from the surgeon/anaesthesia team.
Implementation of the initiative
This project was started with the CHUPORTO team responsible for this type of surgeries and two researchers from LEMA. After collecting anonymous Hospital records, several meetings were held to discuss the intermediate results, allowing physicians to assess the model’s adherence to reality and to use their feedback to further adapt the model to the reality of CHUPORTO. Different techniques were tested, including Decision Trees or Bayesian and classical generalized linear models for dichotomous response.
Results and achievements
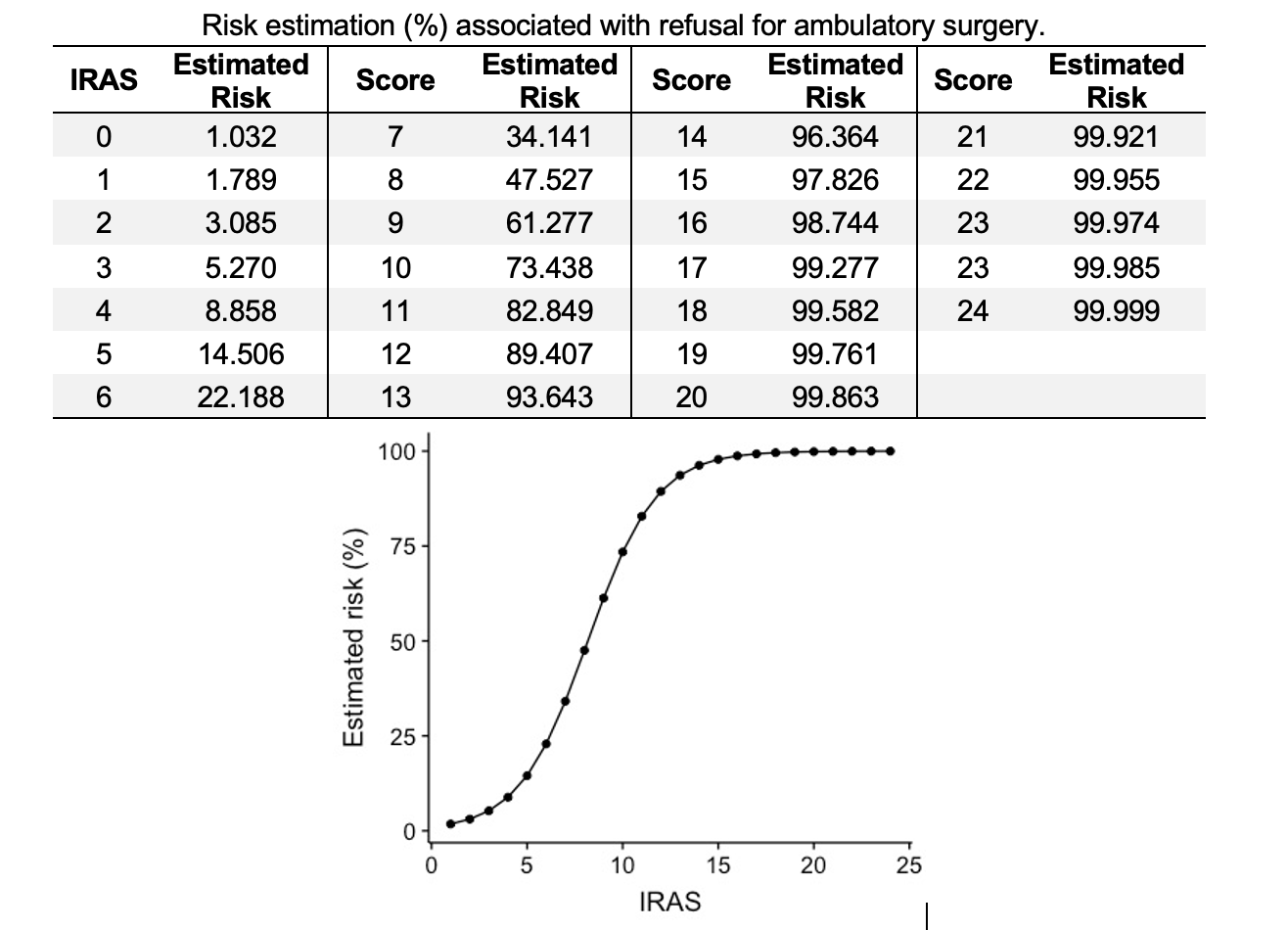
The anonymous records collected from the hospital database consisted of all patients who underwent an abdominal hernia over a 5-year period (2014 – 2018). For each of these patients, a set of 94 variables was analysed. A multivariate logistic regression model was then developed to identify risk factors associated with the final refusal/acceptance decision. A prediction index for refusal in ambulatory surgery – IRAS – was then derived and tested.
From those 94 variables available, the IRAS model uses a set of only 5 variables which will allow the general practitioner to predict, based on such values, the suitability of a given patient for ambulatory surgery. This resulted in a positive predictive value of 93.55% and negative predictive value of 87.10%.
The results obtained seem to indicate that a very good model was achieved, contributing to the reduction of number of refusals and, consequently, to the patient’s well-being. In fact, based on the analysed data, a patient proposed for ambulatory surgery who was declined, has a statistically significant additional waiting period of 11 months until surgery, compared with a similar patient undergoing outpatient surgery.
Lessons learned and replicability
The LEMA team that worked on this project found it very challenging and rewarding. In fact, in addition to all the scientific challenges, being aware that mathematical modelling can help significantly increase patient wellbeing is the ultimate reward.
From CHUPORTO’s point of view, this was a successful venture that resulted in a strong predictive model that is able to efficiently address the patient’s pathologies. This collaboration allows for better patient care and better management of healthcare costs.
The mathematical model can be replicated in other health units. However, as it is based on real data and strongly related to the criteria of the surgical and anaesthesia teams, for adequate adherence to reality, it must be parameterized according to the data from each health unit.
Project team and contacts
Manuel Cruz (LEMA/ISEP), Sandra Ramos (LEMA/ISEP & CEA-UL), João Oliveira (CHUPORTO), Isabel Novais (CHUPORTO), Carlos Magalhães (CHUPORTO), Marisa Santos (CHUPORTO)

LEMA – Laboratory for Mathematical Engineering, School of Engineering – Polytechnic of Porto, Rua Dr. Bernardino de Almeida 431, 4200-072 Porto, Portugal. Email: lema@isep.ipp.pt

João Oliveira (CHUPORTO), General Surgery Department, Centro Hospitalar Universitário do Porto, Largo do Prof. Abel Salazar, 4099-001 Porto, Portugal. Email: joao.oliveira@chporto.min-saude.pt